American neurobiologist Cyndi Shannon Weickert wanted to be a chef. When she found out that her twin brother, Scott, suffered from schizophrenia, she froze her cooking dream in order to be a doctor. In Sydney, Australia, she is now leading one of the most important research programs. And she is confident on a real breakthrough. (Read more…)
© All Rights Reserved
Professor Cyndi Shannon Weickert is the Macquarie Group Foundation Chair of Schizophrenia Research, a joint venture of Neuroscience Research Australia, University of New South Wales, Schizophrenia Research Institute and Macquarie Group Foundation, supported by New South Wales.
Her research is focused on the molecular developmental neurobiology of schizophrenia. She earned a PhD in Biomedical Science at Mount Sinai School of Medicine, in New York City, and completed postdoctoral training at the National Institute of Mental Health rising to the level of Unit Chief of Molecules in the Neurobiology and Development of Schizophrenia Unit. She has lectured throughout the world and contributed to over 110 primary research publications.
Professor Cyndi Shannon Weickert gave me a lengthy interview, in two parts (personal and professional), via e-mail:
Let us begin with your dream of being a “famous chef”. Why this dream? Being a scientist is such a demanding job – researching, addressing conferences, writing… – do you still have time to prepare meals for family and friends?
I think being a chef was among many options for me. I wanted to do something creative, but it could have easily been art or design. In terms of cooking in particular, yes I always loved to cook. I cooked with my grandmother growing up. My favourite dishes to cook are really simple but yummy things.
I love Chicken Kiev which is stuffed with herb butter and cheese sauce, Monterey Jack cheese actually. I like Italian dishes, I make a lot of Italian dishes particularly lasagne and baked rigatoni and I’ve taken gnocchi cooking classes and things like that so Italian is one of my favourites as well.
In terms of eating I like a variety of foods. I especially like the fresh fish and fresh fruit here in Australia. Yes, being a scientist is a demanding job but I still have time to prepare meals, particularly for my husband. Sometimes, though, what I try to do is cook a dish on the weekend and cook it ahead and then just pop it into the oven when I get home from work or I try to make something simple like a grilled salmon or something that’s fairly quick.
I don’t actually have a lot of time to invest in fancier recipes. I still do enjoy cooking and occasionally I will have friends from work over. Sometimes it could be for breakfast, you know on the weekend or dinner occasionally during the week.
The town where you were born was described as so small that “if you drive by it and blink you’ll miss it”. In this place of 2,000 people were (are) there other cases of schizophrenia?
No.
Was your brother’s case the only one in your family? Wy is it important the genetic aspect of this disease?
I don’t think that’s the case so I recently found out that a nephew of mine is showing similar symptoms to my brother and I actually had a great aunt that had very severe delusions and paranoia.
I definitely think that it’s in my family, I guess at what point of the genetic aspect is the disease important, I would say all genes are important, because even if the disease doesn’t run in a family it still could have a genetic basis because each one of us has a de novo genetic changes in our genes that means that we didn’t inherent the DNA from our father or mother but somehow it changed as it was passed down to the child. So you can have de novo changes in genes so I think the genes are always important to consider of course.

Cyndi and her twin brother, Scott, who encouraged her “find a cure” to schizophrenia
© All Rights Reserved
How was your relationship with Scott? You defined him as a “pretty competitive, physically and academically”, always trying to get “the top scores in school”. According to your mother, he was “a happy, curious, adventurous and wonderful boy “…
When we were kids my mom remembers pushing us around in the baby carriage so of course we were twins, so she had one in one seat and one in the other and it was a big job as she was kind of petite woman.
And she said that a lot of passer byers would say ‘hi’ because we were a novelty there wasn’t IVF and a lot of twinning in the 60’s. And she said I was the first one to speak and my first word was ‘hi’ and my brother shortly followed after that with “mommy”. And I think Scott and I used to get into a bit of mischief together as toddlers.
There are pictures of us pulling all the pots and the pans out of the bottom cupboard and playing drums on them. My mom said that one of the things she remembered is that, for example if one of us got a glass of orange juice (say if Scott was given a glass of orange juice) he would say well where is the one for Cyndi so we always sort of looked out for each other growing up.
We wanted to make sure that we each got to enjoy things and to share things, that was really important for us. There was always this balance and sense of fairness.
And then we used to enjoy on rainy days sitting at home playing board games like monopoly and all that because we were the same age, with the same interests, both quite smart and analytical. He was really good in math and engineering as well, so the more complex the game, the better usually for us.
I think when things started to sort of diverge was when boys started to take an interested in me and Scott was a bit protective. I didn’t actually like the fact that he was protective.
I thought he should let me go out and hang out with my boyfriend or to do what I wanted, but he was always concerned that they wouldn’t be treating me properly and that he often would get into fights with them and then I would get into fights with my brother because of it.
I think adolescence was more of a tumultuous time for us and we kind of drifted apart a little bit. And we were very competitive in school so even though we wanted to play together when it came to sort of academic performance we each wanted to outdo one another.
I remember in algebra which is 9th grade mathematics we would both furiously do our homework and be the first one to hand it in the morning and try to answer all the questions the teacher asked. When it came to the end of the year exams I had scored 100% which is every single answer was correct and he was devastated as he scored a 98%.
The following year in the 10th grade mathematics we were competing in geometry and he was so upset because in the final grade as he got 98% and I had got 96%, although he still beat me he was disappointed that he didn’t get the 100%.
And I said but Scott, if you look at the average we were absolutely the same but somehow that wasn’t good enough for him, he wanted to basically be “top dog” I guess.
He was typically the smartest person in the room and yes we did have that sort of competitiveness with each other but also a lot of respect for one another too.
We always had this idea that we will look out for one and other we didn’t want anything bad to happen to each other and we always made sure that the friends wouldn’t talk behind our backs or say bad things about the other twin. Because you know adolescence can be a rough time for people.
So it was OK for us to pick on each other or to compete with each other but we didn’t want other people involved with that, we didn’t want other people to hurt or bad mouth the other twin.

© My schizophrenic brain | Guimarconi
How did you notice that he was acting and saying “strange” things? What kind of things?
Well he would say things like when “I play the Beatles record backwards they are telling me that I should not be going to school today” or something. They would be sending him particular messages I can’t remember the exact content of the messages, but they had messages for him.
And I think at one point around the dinner table he said to me that he knows that “I am the daughter of the devil’ and he was absolutely convinced of it.
I think one time he was threatening my mom and pressing her against the wall so he was not really violent against himself but he definitely turned his aggression towards my mother and that’s when I had to call the police.
When we got to the station, he said that’s not my mom, my mom is Yoko Ono (I think that’s in the documentary). It was very, very bizarre stuff, so it was really very strange stuff obviously Yoko Ono is not his mother.
I think his best friend said to me one night they were at the good friend’s apartment, they were maybe just out of high school and they were sitting around in the living room and they were drinking beer, Scott said “He’s here”. The best friend asked who’s here? And he said “Jim Morrison”.
One of their favourite singers was Jim Morrison from The Doors and they would listen to the Doors constantly. So it was a bit of an idol for my brother these rock and roll stars and obviously Jim Morrison wasn’t in the room. But he was convinced he was there with them partying away. So those were the kind of things, really strange things.
Was your brother ever violent against himself and other people? Who has diagnosed him with schizophrenia, in what circumstances, and based on which signals (hallucinations, delusions…)? You’ve mentioned “wires hanging everywhere in his room”, “playing records backwards (because) they were talking to him”, “trying to get in tune with the voices and messages that were coming on from outside him”…
No, he was never violent against himself. We talked about his violence against my mom. Yes, in terms of the wires hanging everywhere in his room, I think.
There were actually these coloured pyramids of construction paper that he would make. And he would make it 3-dimensional and colour the different faces of the pyramid in different shades like black and blue and red (it was usually bright colours) and then he would put them in strategic positions around his room.
Then he would take sort of hangers and unwind them like connect them from one pyramid to the next pyramid or you know one may be on the table top with the turntable where the record was playing and another one might be on his dresser and another one would be connected to his headboard, and you know there were things pasted on the wall and even had geometric designs over where our cat would eat his dinner.
I guess I don’t know if it was for the cat to receive the messages or to protect the cat. I ‘m not particularly sure what that was all about, but he definitely did a lot with shapes and wires and things like that.

© My schizophrenic brain | Guimarconi
Did Scott ever realise that he suffered from this disorder? What was his reaction when he was informed? Did he accept the medication? How did the disease and the medication affect his body and brain? He did not die of schizophrenia but of “the cumulative effect of other conditions: diabetes, a weakening heart”, your mother said…
Yes, he realised, but not at first. I think his reaction to being informed was that he probably was in shock. He didn’t understand what was happening.
They didn’t have insight or he didn’t have insight in the beginning of the disease and I think that they hauled him off to a mental institution, a State hospital and they injected him with things he said felt like poison to him.
He said he rather be dead then go back to that State hospital with those kinds of antipsychotic medicines that were first available. I believe it was some kind of Thorazine derivative or really strong anti-psychotic that they injected him with and he said it felt like poison and it was awful.
I guess once he started the medicine he got some insight and one time I think I was to blame for one of his relapses because I thought that he was feeling so much better and doing so much better I felt well are you really sure you need the medicine? And so he went off the medicine but then he relapsed.
So that was bit of a shock just seeing all the symptoms come back and see him struggle with it again and it makes me really sad that I suggested that at the time. I guess
I was very naïve in understanding how the disease was managed from a clinical perspective and that one of the worst things you can do is actually come off the medicine and so I emphasise that to all the patients that are in the clinical trial now not to go off their antipsychotics.
He took his medications but he was very concerned that he got the right type of medication and he got the balance and that the doctor didn’t change the medicine once he found something that seemed to work for him.
But the medicine that actually he was on caused a lot of weight gain and so he probably was about maybe 20 kilograms to 30 kilograms overweight and obesity is often a side effect of the antipsychotics, plus he got diabetes.
Also, people with schizophrenia don’t want to go out of the house and don’t really want to exert themselves, so he didn’t have any exercise. He had obesity and diabetes that takes a toll on anybody’s heart and particular on my brothers.

© My schizophrenic brain | Guimarconi
Your decision to move to Sydney had a seriou impact on your brother’s health condition. Because you were twins or because the disease aggravated his sense of loss? At what extend this separation hindered your mutual relationship?
I think that what happened with me moving to Sydney and affecting my brother’s health, I think it was more psychological health, if you will rather than physical health that was impacted.
I think one of the things my brother really appreciated when I was living in the US (it’s a little bit hard for me to talk about) one of the things he really appreciated when I was there is if he was having an issue.
Let’s say with mom, or with his step-father like the step-father wanted him to go out and mow the lawn, he didn’t want to do it or his step-father didn’t think there was anything wrong with his car but he was convinced there was a clacking noise and so he wanted to talk to me about it.
He wanted to get some support for whatever his issues may be with mom and the step-dad and he could call me. He knew he could call any time of day and will get my support.
Even if it was “I think my tooth is yellow and I need to get it fixed” or whatever he needed I would make sure that I paid for or covered it. So, if something was wrong with his car, he would take it in and whatever kind of cheque that he needed I would send it up right away in the mail really with no questions asked.
He might have to make a case for it, like he was convinced that the cushion on his chair that he was sitting on most of the time in the room was bothering his butt and giving him a rash so after he complained too much I said just go out and get another recliner chair so that was just $200.
So I think the thing about is it with Scott, is that I was his safety blanket, I was his sounding board, I was his best friend, I was the person who had unconditional positive regard for him and believed in him no matter what.
So the problem with moving to Sydney was when he wanted to call me I’d be sleeping and if he called me and I’d be in a daze I’d be half asleep, I couldn’t actually grasp what he was telling me about his current problem and quite frankly I’m not sure I really cared that much.
I was in a middle of a dream or sleep state, so I just actually think he got like upset because it was more difficult to call me when there was a complicated code that you had to put in front of all the numbers. And when he when he got the urge to call me I’d be sleeping and I think he just felt that he was drifting away from me.

© My schizophrenic brain | Guimarconi
I do understand how painful these memories are, but can you please tell us about that Thanksgiving night, when your brother passed away?
About Thanksgiving the things I remember we were playing a game actually in the beginning of the day and it was guessing a famous person. You get a famous person in your mind and people would ask you questions and the only way you can respond is to say “yes” or “no”. I think I was imaging that I was the last queen of France.
It might have been Marie Antoinette, anyway the last Queen of France as I just read a book about her. So the question you ask “Is this person dead” and I answer the question basically – “Yes”, and then you ask “Was the person famous – yes or no”, the answer is “Yes”. So you say “Were they were they in arts?” “No”. “Were they in sports?” “No”.
So you have to basically narrow down who the person is through a series of questions, one word answers and forced choices to figure out who the other person is imaging. So my person was the last Queen of France and my brother’s was of course Jim Morrison from the Doors.
That’s who he was thinking about. And so we enjoyed playing that game and then he dressed up in really nice in some of the best clothes I had given him for Christmas years before.
So he had on a really nice polo shirt on and a sweater over it with his docker pants and brown shoes and he looked really good. We had dinner and we actually sat around the Thanksgiving table saying what we were thankful for. I remember my brother saying he was “thankful for his home, thankful for his car, thank you for his dog and thank you for his family” and so it was like simple things in life that he was really thankful for.
I told him that “I was thankful for him because he has given purpose to my life”. I remember that we were talking about travelling to different places around the world together, because a dream of my brother was always to go to England.
He wanted to know what the English people were like (because we were from the “colonies” and we had to fight the English off).
He was wondering if the English people, because they have such a sophisticated accent to us (to our American ears) they sound so proper, he was wondering if the English people were actually better stock then the Americans, about the same stock, or that their actually somehow substandard to the Americans.
So ‘better, the same or worse” than us Americans is what he was going to try to determine and he was doing his “research”.
So finally his dream comes true, and I get my first chance to go overseas to go to England for work and tell him Scott you have to get your passport as you are coming with us and so he comes. We actually landed on 9/11 and this threw my mother into a hysterical fit because it was 9/11/2001 but we weren’t hurt in anyway.
Scott decides to go about his research and he does it at the pub, so his meeting English people at the pub and he’s kind of chit chatting away about English culture, customs, the history, different things that he can think about over beers and after a week-long of this “research” that he is doing and touring London on a double decker bus with us and going to see London Palace and different things in the area.
Walking around the streets of Oxford he concludes, at the end of trip, that he “thinks that the English people are just about the same as American people’.
On Thanksgiving what happened was I was saying where would you like to go in the world next and he said what makes you think we’re going to go touring the world? I said, well Scott you know when we cure schizophrenia; everybody is going to want to hear how we did it so, so we are going to be wanted to travel all around the world.
I’d said I’d get up on the podium and tell them it was all because of you that I did this. Then Scott followed and I am going up on the podium and say it was all because of you Cyndi.

© My schizophrenic brain | Guimarconi
“We have to believe in things that are beyond science, beyond our human capabilities and take things on faith”, you said. Is faith important, and how do you combine it with science?
So I think that the issue about things that are beyond science has to do with the idea that we as human beings have a limited capacity to understand and reason.
We are limited based on the human brain that we have. And I think that you have recognise that there are forces that work in the world and the universe that is beyond our capacity to understand.
The way I reference this spiritual being, or this otherness, this force really that I consider the force of goodness is, is it embodies God and embodies something beyond our own limited human resources.
I think that you know the fact that Jesus walked on this Earth and tried to portray to humanity some semblance of what God was like with unconditional positive regard and this ability to sacrifice oneself in pursuit of others and to forgive others and to love one another.
All the emphasis is on things that are really selfless and that’s the kind of spirit I think that perhaps is like godlike or is Jesus like. And I realised when I was going to College that I wanted to be like Jesus and rather than me choosing my life path and saying what I wanted to do all the time and putting myself first.
I felt that I should let go of those desires and let God lead me in my path forward and I think that’s how I was driven to get a PhD perhaps instead of an MD, that’s why I went to New York City as opposed to going anywhere else for education because I prayed about these things.
That’s why I met my husband I said “God I have done a really bad job at picking out boyfriends and partners so could you help me with this one?” And I decided I wasn’t going to make judgements about the fellow that he presented to me, but yet I was going to try give him a chance.
My husband is very different than me, he’s very introverted and he’s very shy not someone that I would have gravitated towards naturally, but I felt like OK maybe this is the guy God thinks would be a good partner for me in my life.
I think if you sort of decide that your life is in God’s hands or is beyond your own control in a way there are forces at work that can guide and shape your life and that you realise that your mission is not about making yourself bigger and better but making the world a better place and showing compassion and love.
Those things are really important in terms of setting a moral compass for your life and recognising why you are doing the science, not just to be famous. Even though I said I wanted to be a “famous chef” I know but it’s not about really the fame, the most important thing is about making a difference in those lives of people that are suffering, that’s where the real importance lies.

© My schizophrenic brain | Guimarconi
Why did you decide to become a doctor and was this decision directly related to your brother’s disease? Determined, as you said, “not just to write prescriptions but to understand schizophrenia at its root causes”, when did you find out that it would be a mission for “several generations”?
I think that any decisions, any life decisions, like what to do with your career is complex and I definitely decided to become a doctor because my brother suffered from schizophrenia that was the primary reason. Another reason I wanted to study biology is because I fell in love with biology at the Community College.
I thought it was really interesting when the instructor had explained to me how diabetes occurs in individuals. I thought the same kind of underlying biological and molecular understanding of a disease like diabetes could be applied to a disease like schizophrenia.
I think I also had an aptitude for analytical thought and I liked mathematics so it was natural I would gravitate towards the sciences. And I had the passion and the interest to apply it to a disease that I felt really needed some better answers than the ones that were available at the time that my brother first got diagnosed.
Well in terms of the contrast of becoming a famous chef I think that the idea that I was trying to portray there was that if I didn’t feel this compassion for my brother and this need to work on this disease that I might have been more inclined to being in a field that was creative that still involved or had a lot to do with interaction with people or making other people happy.
I really like cooking and food and sharing with other people. But it easily could have been fashion or architecture or something with a lot of design element to it, I think this creative potential is what I was trying to portray and I guess I do certainly have a love of good food and eating (laughing).

© Schizophrenia And Art
“One of the things that we know about schizophrenia is there’s no culture, no gender, no IQ, no family that’s immune to it, it can strike anybody”, you said. What is the right definition of this disease? What do we know and not know yet?
Well, the right definition of the disease is one that’s been cultivated or refined by psychiatrists over the last 100 years.
And they have certain criteria you can look up in manuals like the DSMIV or the ICD10 and it needs to meet set of criteria like hallucinations and delusions or disorganised behaviour, thought disorder or negative social symptoms like withdrawal, lack of motivation so there is a whole combination of symptoms that is used to diagnose the disease. Usually are gleaned from clinical interviews, so with interviews between the doctor and the patient.
What is the main breakthrough since it was diagnosed for the first time?
Probably the first major breakthrough was the chance discovery that injecting Chlorpromazine or its equivalence would calm patients going for surgeries and then apply this drug to schizophrenia and blocking the hallucinations and delusions.
I say this is a chance discovery because it was in the 1950’ s that they were actually using chemical dyes in surgical procedures and they noticed that it had an anti-anxiety effect and some astute doctor decided to inject it into the “crazy patients” in the hospital ward and found that it was actually a benefit.
It was because the patients with schizophrenia became more what you may call “manageable” that they able to really shut down a lot of the large psychiatric wards that they had especially in the United States and perhaps throughout the world. But, I am not really sure what the status is of with large institutions are in other countries.
Are the symptoms common to all patients or not? Please give us as much detail as possible about the process that leads to schizophrenia. When does the first episode usually occur? Is this a mental illness of young people in opposition to Alzheimer?
The symptoms are the same or overlapping or similar, certainly a core group of symptoms. I think that one of the first signs of schizophrenia is social withdrawal. You are asking if isolating themselves from relatives and friends is a signal is common and I think it is a very common first system.
What happens is that adolescents can also have mood swings and they can be actually be very distraught like if a boyfriend breaks up with them or they don’t make it on a baseball team so social issues are paramount to adolescents.
But this thing that sort of creeps up on people that then go to develop schizophrenia is lack of ability to want to socialise at all. To retreat into one’s bedroom to find it actually very intimidating to be around one’s peers.
And it is not just one night or a weekend it is actually something that lasts for months so it’s not like they can snap out of it necessarily and that is perhaps one of the differences, that it’s fairly persistent.
The first episode can usually occur around late adolescence so 18 to 22 so the disease can be first diagnosed when they are just finishing high school although the prodrome, this social withdrawal and the drop in scholastic scores or academic achievement, can happen 2 to 3 years earlier so we are talking 15 to 16 years of age but often times it is when a son or daughter will go away to college the first time that it first becomes manifest.
There is in rare cases of childhood onset of schizophrenia but that is thought to be less than 1% of the entire population of people with schizophrenia. And of course it’s a mental illness of young people as opposed to dementia which is usually going to strike in the later decades of life 60’s, 70’s, 80’s for example.
The difference is that an individual with schizophrenia is going to be robbed of their life potential after the family, the community, the government has put money into this individual in terms of education and socialisation and they are actually not able to use that investment to be able to go to college, gain a career, to hold down jobs to get married and to be a productive member of society, that then gives back.
So the real tragedy is actually the loss of potential for these people that are suffering from schizophrenia.

© Schizophrenia And Art
How do you explain the method and the main focus of this “molecular, cellular and cognitive development” research? How hard is it to work with brain tissues? How many people are involved in the project (scientists, volunteers…)? How are patients reacting?
The main methods is that we use brains from people that have passed away and they have the diagnosis of schizophrenia compared to controls and it takes an understanding of the DNA the human genome and cellular neuroanatomy.
We basically look at the patterns of gene expression in the brain, so you have to have high level training in molecular biology and in neuroanatomy to put the molecular changes in an anatomical context and have to be able to recognise different cell types in the brain and how they may be failing to communicate to one another.
I guess that it is not that it is physically hard to do; it is the theory behind it takes a degree of study and I think there is also quite a bit of variability from one person to the next.
It’s not like a controlled experiment and so you have to take potential confounders into consideration with your statistics how you analyse and interpret the data.
I think one of the problems with using human brain material is that historically there has been a lack of consistency in findings from one laboratory to the next.
We are overcoming that now in the field by using larger and larger groups of subjects so that we may have in our collection 38 to 40 brains of people with schizophrenia and age-matched and quality-matched controls. So, I would say it is getting easier but I don’t think any kind of researchers ever would say it was particularly smooth sailing.
I wouldn’t call it easy, but I think it’s definitely more manageable now perhaps because we have more tools at our disposal then we used to.
By tools I mean things that we can do through a high put through way instead of just looking for example looking for one molecule at a time, sometimes we can look at thousands of molecules at a time in a single experiment.
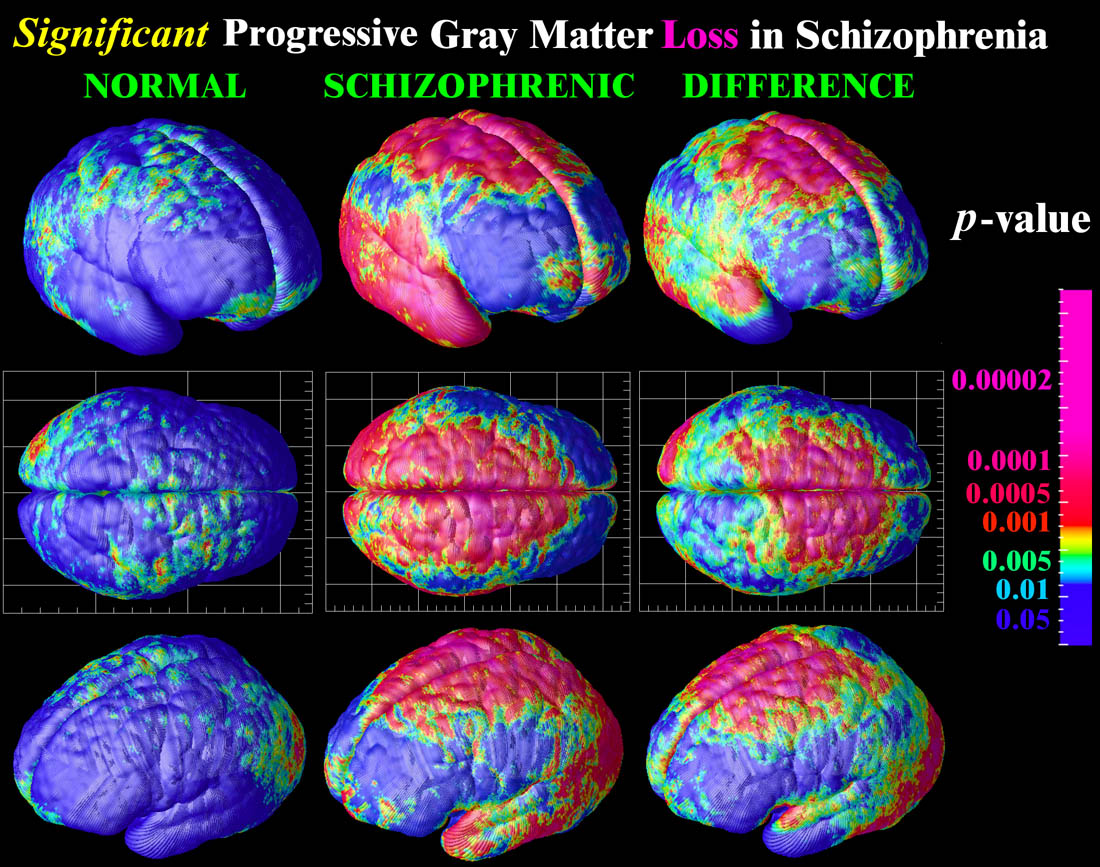
More modern theories suggest that the cerebral cortex, that normally controls the dopamine neurons, is weak and that the disease really begins in the cortex. In the past, neuropathologists looking at the cortex thought that there was no evidence of weakness or cell damage anywhere in the brain.
One of the most exciting discoveries of modern neuropathology is that there are in fact cells that are damaged, but they are small inhibitory neurons in the cortex and may have been missed by earlier investigators. The fact that cortical inhibitory neurons are damaged is the most agreed-upon finding in the field today.
We were drilling down and examining molecules made by cells to search for even more specific neuropathology, trying to uncover the possible causes of the demise of inhibitory neurons.
We wanted to use the most current technology to examine thousands of molecules at once with extreme sensitivity to see what the brains themselves could tell us about how the molecular environment of the cortex may be different in schizophrenia compared to controls.
We coupled this discovery-driven approach with a hypothesis driven approach. We re-examined an old theory that there was no gliosis in the brains of people with schizophrenia (as would be predicted if there was cell death and neuronal damage).
We used modern staining approaches and the largest number of samples ever studied and hypothesized that if we looked in the right way we would in fact detect gliosis.

© Schizophrenia And Art
What have been the main findings of your research so far?
First, that there was indeed evidence of gliosis in the cortex. It was the small glia, the microglia, that were elevated in the brains of people with schizophrenia. These glial cells are the resident immune cells of the brain and an increase suggests that they are reacting to neuronal damage.
Second, we found several types of molecules typically produced by immune cells, known as cytokines, to be greatly increased in the cortex of people with schizophrenia.
Both these lines of evidence suggest that there is an active process of cortical damage occurring in the brains of people who suffer from schizophrenia. We found a large proportion, around 40%, of the people with schizophrenia fell into this high inflammation group.
Schizophrenia does indeed have a biological basis. Our findings mean that increases in cytokines reported in the blood of people with schizophrenia may be linked to increased cytokines and immune activation in the brain.
We may now be able to develop a blood based biomarker to identify those with neuroinflammation as part of the pathophysiology of this disease.
Importantly, treatments being developed to treat neuroinflammation may provide novel therapies for people with schizophrenia. Since the response to neuroimmune therapies can be dramatic, we may see restoration of function and some people “cured”.
It is also likely that there will be different reasons for neuroimmune dysregualtion in different people with schizophrenia and we should be thinking about developing ways to distinguish these and to target treatment.
I would suggest user a laser guided, instead of a sledge-hammer, approach. Also, we as people interested in treating those suffering from schizophrenia, have a lot to learn from other scientists and doctors who have already been treating neuroimmune disorders, such as neurologists and immunologists.
Why is Australia the centre of your research? When did the project begin and how do you get the necessary funding?
Well Australia is the centre of the research that I do because they recruited me here to Sydney to be a leader of schizophrenia research. And it’s not that research is not occurring in the United States or other countries it just has to do with you know I am only a small portion of all the research that is happening internationally and around the world.
So it is only the centre from the perspective of the work that we are doing and I was recruited in 2006 and the main contribution is from the NSW Government, I mean the State Government (not the Australian Federal Government) with contribution from the Macquarie bank, University of New South wales and Neuroscience Research Australia.

© Schizophrenia And Art
Is there a deadline to reach a conclusion – and at what stage are you now [in 2012]?
Our clinical has actually just finished the end of August we had our last participant we reached our target number for our subjects and now we’re just checking all the data shoring it up to make sure it is accurate before we break the blind.
There is not really a deadline to reach a conclusion. I think research has its own idea of when the deadline is going to happen.
Usually with research what you do is make a discovery and that usually leads to more questions. So I don’t think research ever really has a deadline per say. There are the project deadlines dates you know time points that we want to finish particular projects but the research itself I anticipate will be going on for a very long time.
However, I think that while that is the case and there will be long term research goals in the basic neuroscience of schizophrenia, but I think that we will be able to deliver new therapies in the shorter term perhaps without understanding the complete mechanism behind the way the treatments are working I think we have the responsibility to the patients to also apply therapeutics in the here and the now instead of waiting for 10 to 15 years for all the research findings to come out.
Why is the pharmaceutical industry not investing more on drugs for mental illness? Raloxifene, for instance, the drug that you have been using had positive effects on breast cancer, so it is not a medicine conceived specifically for schizophrenia.
I think that the Raloxifene is actually being marketed as an osteoporosis drug and when I asked them about their interest in Raloxifene for schizophrenia they said that’s the “bone peoples drug” not the “brain people’s drug”.
So I can’t really tell you why they are not interested in it. I think the decisions that drive a big pharmaceutical company or certainly the whole industry are really beyond my capacity to comment on.
Can you detail the effects of Raloxifine’s therapy on your patients? Is this therapy already being applied in hospitals?
That’s what our clinical trial is about. Is this therapy applied in hospitals? No it’s not currently being applied. Perhaps they are waiting on the outcome of our clinical trial and of others like it.
One thing important to consider is we do not expect every single person with schizophrenia to get benefit from this therapy, we only expect a subset to be true responders about 20% of people with schizophrenia we expect to get a beneficial effect particularly on cognitive and emotional symptoms of schizophrenia.
So the individuals with more negative symptoms and the more intellectual difficulties may benefit the most.
“I decided the best way to help was to understand what was causing the disease so that we could come up with therapies and treatments to deal with the root of the problem, rather than just treating the symptoms – that has been a quest that I have been on for the last 20 years”, you said. Are you confident that you will be able to find a cure in your lifetime?
We will move towards a more personalised, preventative approach to treating people with psychiatric problems. As our biological understanding grows, we will be able to reposition more drugs to trial in schizophrenia. We will develop biomarkers to help tailor treatments.
I think that the most important thing is that there is not going to be one cure for schizophrenia ever. There’s going to be cures for schizophrenia and I am confident that I will discover one of those in my lifetime.
Your husband changed his medical interests (from animal social animal behaviour) to take the quest of your life – how is it to work as partners?
Well sometimes it’s fantastic and we really feed off each other and at other times he drives me crazy. So, it feels that we are working non-stop of course through breakfast, lunch and dinner together where we just talk about work.
We currently don’t have children and I would say the work is definitely a cornerstone of our life together but we both really enjoy it and it’s something that sort of we see as a quest and as an interest.
It’s not only our work, it’s our life, it’s our hobby, it sort of consumes us we can spontaneously launch into some analytical conversation and then be talking about relatives or upcoming vacation the next minute, so it’s sort like weaved into our being. Then it’s good because it’s not like you really feel that work tears us apart from one another.
When he is doing work he is not taking himself away from me because when he’s doing work it’s actually work that we are doing together. So you know sometimes when you have a partner that’s working and you’re feeling oh he’s ignoring me.
I don’t feel like that with Tom, he is working for us or we are working together on a problem and I guess that it’s a different way to think about it.
Of course what we do take time out to relax a bit together is to either take a little trip, or we like to get massages or we like to do wine tasting or we like to visit the family. We used to canoe a lot when we were in the States but there are not a lot of places to canoe here in Australia. So some beach walking, we like that. Swimming, we do, Wi fitness we do, things that break the work up and we also either go shopping or go to the gym.
An Egyptian academic recently described the legacy of Mr. Hosni Mubarak as “schizophrenic”. I asked him to use another other word. At what extent the use and abuse of these metaphors affect patients and their families?
Well I think that with people with schizophrenia get a label and there is a lot of misconceptions about what schizophrenia is and schizophrenia isn’t.
I don’t really think we will get a better understanding of schizophrenia as a biological disease until we can really offer therapy and have the people be relieved from this terrible suffering and re-emerge as themselves then perhaps then we will understand that schizophrenia is really a biological disease like diabetes that needs to be treated accordingly.
I guess I would hope that the disease label is something that can be looked at differently in the future once we develop appropriate and life healing therapies.
Cancer and depression are not so “demonised” by society as in a recent past, but not yet mental illnesses such as schizophrenia, bipolar disorder or OCD (obsessive–compulsive disorder). What shall be done?
I think that one of the things you have to keep in mind is that people that suffer from schizophrenia don’t want to be integrated to society. They don’t really want to be integrated with people.
So I think you really have to cure the disease or cure the root cause and then try to rehabilitate people so they can re-enter and I think that’s an important part of any therapy.
A lot of times these people have been estranged from society for decades and if we are going to be able to offer therapies either pharmacological or through brain stimulation it’s going to repair their brain and repair their function that we may also need to support their social reintegration.
I think awareness that it is a biological disease can help with the stigma in a way because the people aren’t blamed for their disease, but I think that until we really have the answers, therapeutic answers they will be having a difficult time getting through the stigma or getting people with schizophrenia to want to be more social.

© neura.edu.au
Parts of this interview were included in an article published in the Portuguese newspaper PÚBLICO, on November 11, 2012
